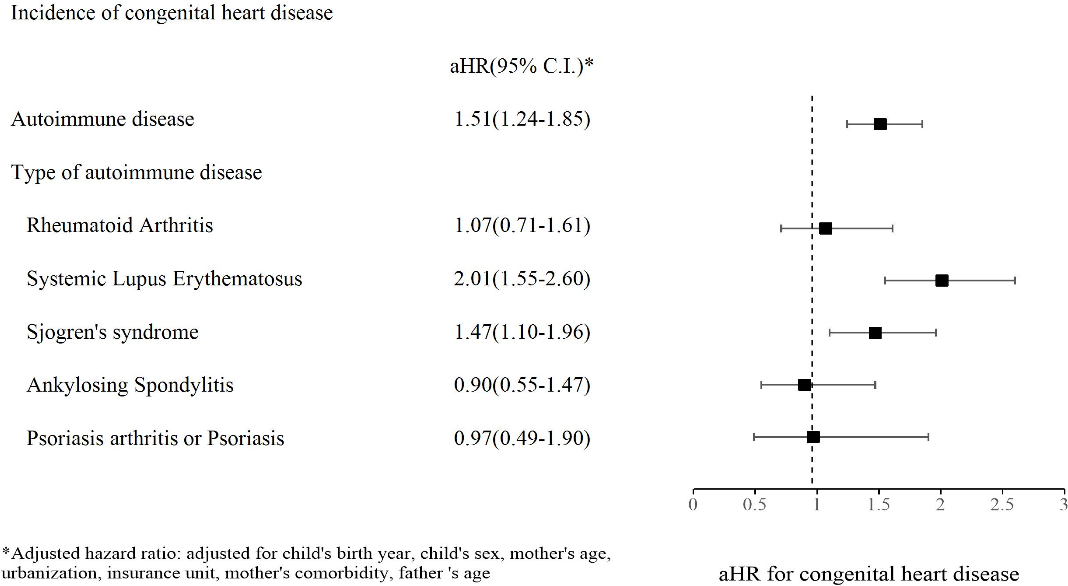
Objectives Very few investigations have explored the association between CHDs in offspring and mothers with autoimmune disease. In this study, we aimed to explore whether maternal autoimmune disease increases the risk of CHDs in newborns. Methods We analyzed 4780 offspring with maternal autoimmune disease and 9416 offspring without maternal autoimmune disease matching 1:2 with age and sex between 2009 and 2016 from databases including the National Health Insurance program, birth certificate applications, cause of death data, and Maternal and Child Health Database, which is managed by the Health and Welfare Data Science Center (HWDC) in Taiwan. Birth year, birth weight, gestational age, the children’s sex, mode of delivery, congenital defects, urbanization, insurance unit, maternal and paternal comorbidities, child or parents died within one year after birth and medication exposure during pregnancy were selected as covariates for further multivariate analysis. Also, multiple Cox regression analysis was performed to evaluate the adjusted hazard ratio (aHR) of CHDs. Results The incidence of CHDs was 5.35 per 10000 person-months in autoimmune mothers. The result of the multivariate Cox regression showed that the children whose mothers had autoimmune disease had a 1.57-fold risk of CHDs compared to children whose mothers did not have an autoimmune disease (crude hazard ratio: 1.57; 95% CI, 1.29-1.90, aHR: 1.51; 95% CI, 1.24-1.85). Conclusion Maternal autoimmune disease might be a risk factor for developing CHDs in offspring, especially in mothers with systemic lupus erythematosus or Sjogren’s syndrome. Further research is warranted to investigate the possible pathogenesis mechanisms of this association.