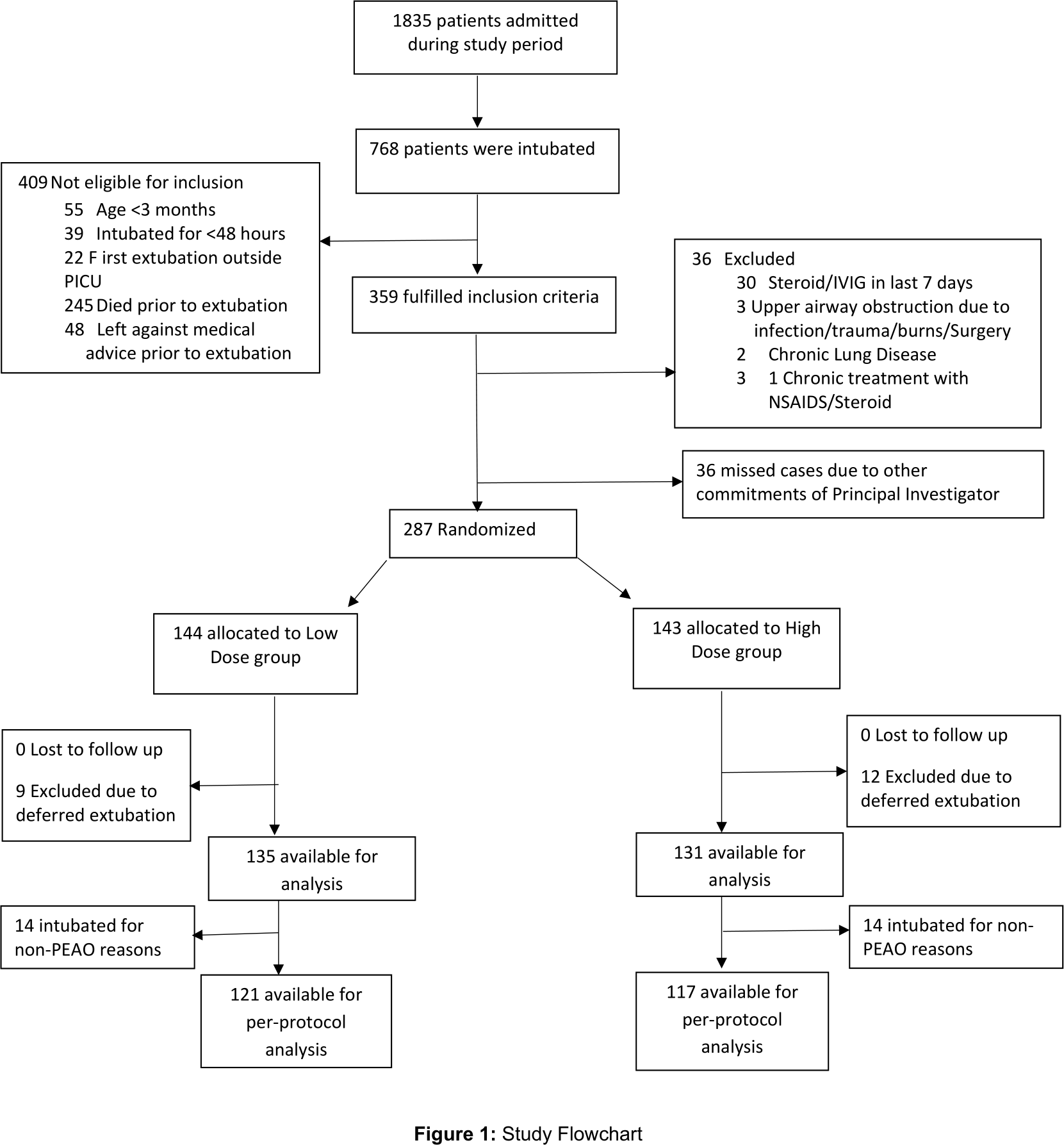
Objective: Multi-dose dexamethasone pretreatment prevents postextubation airway obstruction (PEAO), however, its optimal dose in children is not known. We planned to compare effect of 24h pretreatment of low dose (LD) (0.25mg/kg/dose) versus high dose (HD) (0.5mg/kg/dose) dexamethasone for prevention of PEAO. Design: Stratified (for age and intubation duration) randomized open-label non-inferiority trial. Setting: 15-bed Pediatric Intensive Care Unit in a tertiary care teaching hospital of a lower-middle income country. Patients: Children (3mo-12yrs) intubated for ≥48h and planned for first extubation over 26 months (Feb’17 to Mar’19). Children with preexisting upper airway conditions, chronic respiratory diseases, steroid or IVIG therapy in last 7 days, gastrointestinal bleeding, hypertension and hyperglycemia were excluded. Interventions: Low dose (n=144) or high dose (n=143) dexamethasone (q6h) for 6 doses. Extubation was planned after 5th dose. Measurements and Main Results: Patients were monitored for PEAO (Westley’s Croup Score >4) for 24 hours. 238 patients were included in per-protocol analysis. 78 patients (33%) developed PEAO; both groups were similar (LD, 41/121, 34% vs HD, 37/117, 32% p=0.71). Risk difference of LD vs HD touches the non-inferiority margin of 0.12 and hence the overall result is non-significant. Incidence of reintubation was also similar (LD, 10/121, 8.3% vs HD, 9/117, 7.7%; p=0.87). Intubation for more than 7 days was an independent risk factor for development of PEAO. Conclusions: Multi-dose 24-hour pretreatment with low dose dexamethasone is not inferior to high dose in preventing PEAO and reintubation among unselected patients in the studied clinical setting. Multi-centric trials with larger sample size among children at high risk of developing PEAO are needed.